

Relevant & Core Issues in ME/CFS & Long Covid in Research, Care & Culture.
Part One

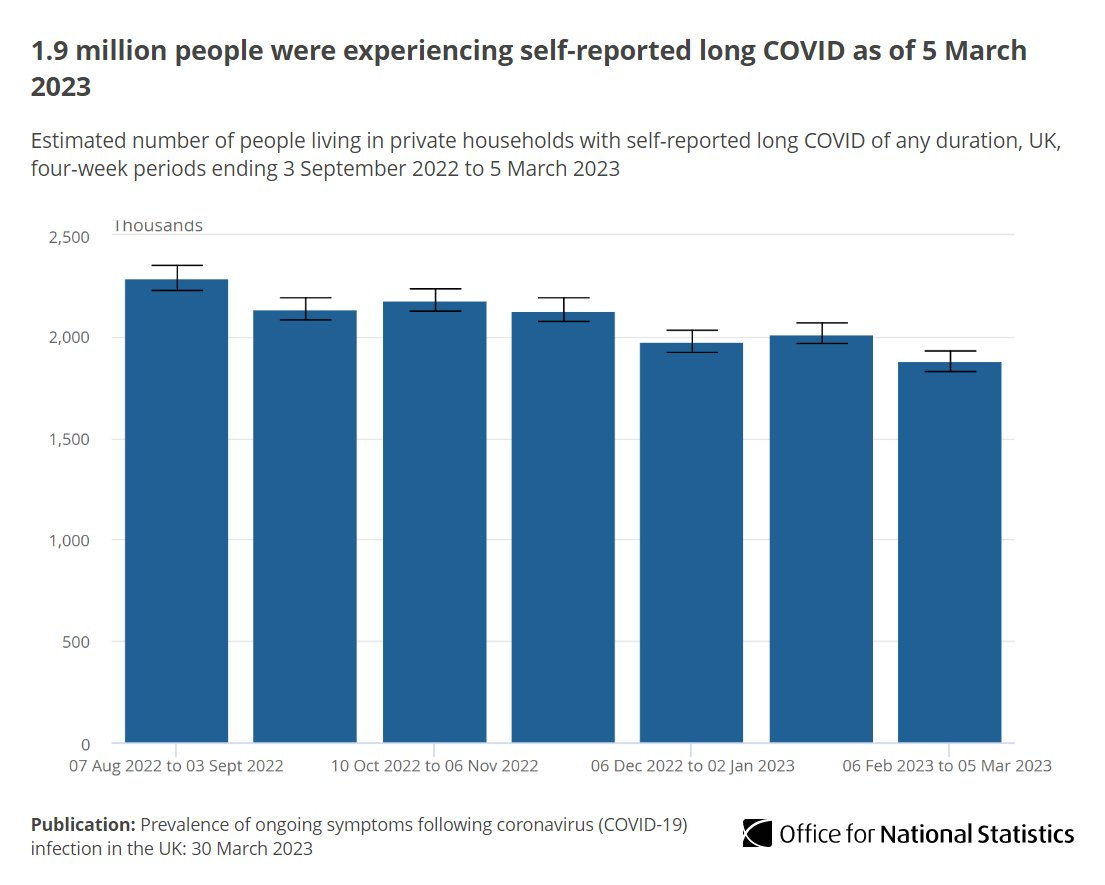
We are facing a Public Health disaster on a vast scale with the rise of Long Covid. The REACT2 study in June 2021 estimated there are 2 million people with Long Covid, the latest & last ONS figures in March 2023 states there are 1.9 million people with Long Covid. This isn’t a problem going away. For some context this is the size of nearly 2 Birminghams.
In 2021 the Academy of Medical Science estimated that 5000-20000 people a day could contract Long Covid if Covid is let loose through the population on current projections. The extent of the problem in the UK is due to issues that arose & are still present in the treatment & handling of ME/CFS in culture, funding & patient care. It is vital to open a dialogue, collaborate with ME/CFS researchers & increase education in post-acute viral conditions – both medically, publicly & politically. We need efficient policy.
1. Lack of understanding of post-acute viral conditions in health care professionals.
This is due to the lack of education & training in Medical School & underfunding in Professional Development. A study at Manchester University Medical School[1] in 2015 showed that ME/CFS gets no official time in the syllabus. Here are some of the students comments; it would be a
“a wasted week”, “mere tiredness” “like everyone gets knackered no one really cares” “brushed under the carpet”
The condition was vaguely ascribed to be psychosomatic and based on deconditioning. 1 source said they had 5 mins of training. Numerous studies have shown that many GPs and Specialists do not believe in the biological reality of post-acute viral illness.[2] [3]
It was therefore inevitable that the medical world was not prepared for Long Covid, even though every major viral outbreak has had post-acute viral consequences; zika, ebola, SARS, MERS.
"At the beginning of the pandemic, we didn't know what the long-term sequelae of a Covid infection would be," says Heightman, a consultant respiratory specialist. "We thought it would be like flu, it would all just go away, and be fine."[4]
20% of visits to the GP are for MUS (medically unexplained symptoms)[5] and Drs need more training in how to deal with patients with these conditions.
“There’s nothing I can do about that”; “What do expect me to do about it” “ I will diagnose you with ME and Fibromyalgia and discharge you now” “It’s often caused by emotional issues like when your mum dies” “I won’t refer you to a specialist” “ Don’t talk to anyone else with ME it will make you worse” “Yes you have Long Covid, read this book, your discharged now” GP & Consultant experiences of C. Higham
2. Lack of understanding of conditions that are connected or arise through post-acute viral illness ie MCAS, POTS, hEDS, EDS, Fibromyalgia, Autoimmune, OT, Gut Dysbiosis, GAD, collagen issues, Small Fibre Neuropathy.
ME/LC are multisystem, complex conditions that also present differently in individuals. Many of these conditions form a diagnostic soup that are not well funded or understood on the ground at the GP or Consultant level. The research is there but has not trickled down. The compartmentalisation of medical care also means that patients are repeatedly referred to different specialists forming an endless cycle where no one takes responsibility. The other pathway is because the conditions are not understood the patient is dismissed and left without medical care.
We need a complex multidisciplinary system for patient care and the ability for specialists to hold a complex view of co-concurrent and co-morbid conditions - with a possible diagnostic tunnel with multiple tests for each effected area of the individual.
“Over 90% of patients will respond to treatment, thus heightening the tragedy of delays in diagnosis and treatment. As it effects so many body systems, a multidisciplinary approach is recommended, but there is no such service available in the NHS for UK patients.” POTS UK[6]
3. Lack of joined up care to manage specialists (if you have any).
This can be exhausting when severe fatigue is present. A 1-point nurse, like in other complex conditions such as Parkinsons[7] or Cancer (Macmillan)[8] to coordinate care, medical & psychological support, occupational health, help with forms etc would be invaluable. This would stop many people falling through the cracks.
4. No practical help or social care.
Even if there is no medical treatment Drs underestimate the intensity & debilitation of Long Covid & ME/CFS fatigue.This isn’t even the right word as it’s descriptive and not related to the biological pathology. Many people are struggling to wash, sit up, cook, clean and look after kids and work. This is reflected too in some family and friends because it is an invisible illness & you can look well. We need funds or scheme for cleaners, meals delivered, childcare.
Long Covid mainly effects women between 35-49, this is the sandwich generation that often have children and parents to look after. It is a devastating experience to be disabled and not be able to look after oneself or family – both for the individual, family and children. This makes women very vulnerable and there are utter horror stories of women on the FB forums of how hard and impossible LC is.
After I collapsed with hypoxia with Covid I couldn’t move from my bed. I was stuck under an eye mask in a darkened room for 3 months, unable to look after my 2 children (both who have SEN) who needed home-schooling & care. 7 months later I still can’t cook or clean or walk down the road. Long Covid has made me dependent on my families care and support financially and physically just to get through the day. C. Higham
5. Problems with finances and the benefits system
This is especially for key workers in Long Covid as it has not been made an occupational disease. People with both conditions are often asked to leave their jobs, let go and face severe financial stress and hardship. There is also the issue that if you live with someone you do not receive financial benefits or aid. All financial independence disappears which again can leave women in a very difficult and vulnerable position. Patients are not usually in a position to take legal action due to fatigue. You need an excellent & priviledged family and friend support system to be able to cope.
In the call for evidence from the APPG for key workers with Long Covid [9] showed 1 in 10 had lost their jobs and 1 in 5 had been off work for more than 12 months. There was also repeated evidence of lack of ongoing financial support. The APPG for Covid are calling for a compensation scheme and ongoing financial support. In the UK only 3 conditions are protected in the Disability Equalities act: MS, Cancer & HIV[10].
From the point of diagnosis people with MS, Cancer and HIV are protected from under the equality act . It gives them significant protection from diagnosis. Paula Cole, Solicitor.
Any other condition comes under the broader definition as to whether the illness lasts 12 months and is assessed on a case-by-case basis. This needs to change in the UK and not just for Long Covid but for ME/CFS and other energy limiting conditions. The Equality Act needs reassessing on a much broader level. Individual who are severely fatigued cannot do individual tribunals & the mass of paperwork and evidence required, this is an unjust burden. What happens in both conditions due to not being under disability protection is that the individual uses up all their sick leave, holiday leave and then this triggers absence management policies that can lead to job loss, discrimination and financial instability. This leads to untold stress and worry. Workplaces and GP surgeries which are private practices need more and clearer guidance and support on LC/ME employment policy. The other issue is Universal Credit and PIP are not fit for purpose for ME/CFS/LC.
President Biden[11] on 26th July 2021 stated that Long Covid patients in the US “will have access to the rights and resources that are under due under the disability law.” We have yet to see that in the UK. It is likely that the experience of LC will change the disability system in the US[12].
6. Be your own doctor, advocate & self medication.
Due to the lack of care that very often occurs patients with the least energy, both physically & cognitively they have to often research their own condition to try and get better. Both communities can spend vast amounts on supplement and special diets. People also self-medicate with prescription drugs in a desperate attempt to get better.
There are also a lot of pseudoscience sharks who go for people with an MUS and who charge a lot of money to vulnerable patients ie Gupta, Lightening Process, REACT[13]. What has occurred especially with the introduction of the Internet is bottom up or citizen medicine where groups of fellow sufferers come together to diagnose, support, campaign for themselves as a community. They have to advocate to be recognised, to be given protections, for research and to be treated with respect and for people to recognise the reality of their condition. This is pretty amazing and awful as we have the most knackered people on the planet having to do this. LC is also not officially counted[14] or registered and until this happens the Government won’t include it in its policy decisions and the public will be unaware of the risk they run for both adults and children.
7. Both communities have an increased risk of suicide.
There are studies in ME/CFS not Long COvid - yet. ME/CFS patients are x7 at more risk of suicide[15] – this is not due to the condition but the lack of care and dismissal that happens. We are seeing this anecdotally in FB Long Covid groups. See the case of Heidi Ferrer (Dawsons Creek Writer) wife of Nick Guthe[16].
8. The BIG ONE – Lack of Public Funding in Biomedical Research in Post Viral Conditions
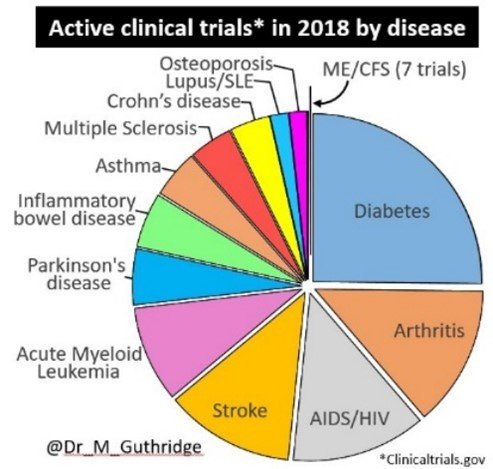
The problems that arise in both communities are a chain of connecting causes and conditions and it can be tracked down to one foundational cause – lack of public funding into biomedical research of post-acute viral conditions. This is especially true in the UK. Dr Mark Gutheridge[17] in 2018 analysed the data and determined ME had the worst quality of life[18] than any other chronic condition (also researched by Dancy & Friend) including Cancer and the quality of life is equivalent to stage 4 renal failure and it gets the least scientific research and clinical trials.
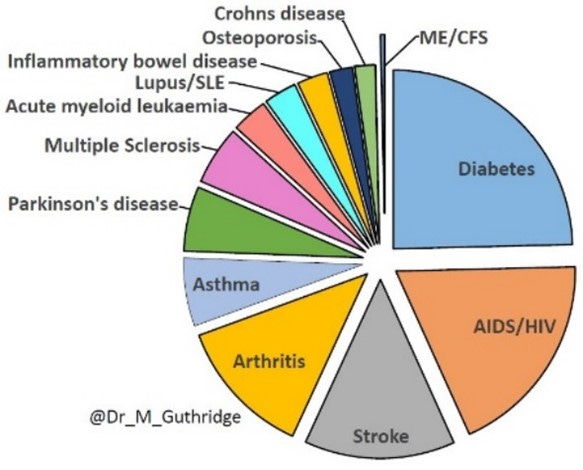
Less than £1 per patient with ME is invested in funding yet it costs the UK economy £3.3 billion a year. Yet on biomedical funding there is no public funding it all comes from charities and donations and patients are asked to fund their own research. This is due to the dominance of the behavioural model or Biopsychosocial[19] (BPS) school that dominates the UK for funding. Which essentially see’s ME/CFS as a psychiatric disorder of mass hysteria with no pathophysiology/ underlying disease mechanism[20]. Can you imagine getting Muscular Dystrophy, Cancer or Lupus and being sent to a Psychiatrist for primary mental health care as your disease doesn’t really have a physical basis!!!??? The current research in ME/CFS especially in the States has robust evidence for a biological, pathophysiology as stated by Standford and Harvard’s Lipkin and Komaroff[21]. Yet the battle for funding in the UK is still a disaster for biomedical research. The NICE ME/CFS guidelines have changed and for the better which should help create the culture change we need - but this movement is slow. Yet NICE is determined that they are 2 separate conditions. This is partially true but around 50% of people with Long Covid meet ME criteria and the most are not getting the better protection from the ME Guidelines.
If anyone deserves an apology it is the people with ME/CFS, many of whom have experienced years of being told that their symptoms are “all in the mind” and given no meaningful medical management – mainly as a result /of the dominance of the psychosocial model of causation. As a result, progress involving biomedical research into the underlying cause of ME/CFS has been severely hampered. The NICE draft guidelines (November 2020)
The ME Association further clarifies, “The reason why people with ME/CFS feel angry and let down by the medical establishment stems from the fact that almost all biomedical research until recently has been funded by donations to the charity sector. Almost all government funding has gone into research based on a flawed psychosocial model of causation.[23].
The history of ME remains one of the worst examples of unacknowledged institutional abuse in modern times. Valerie Eliot Smith, 2019[24]
This institutional failure has had profound ramifications for the understanding of Long Covid[25] as we do not have the history of biomedical research in post viral-acute Illness to fall back on. We have caught with our pants down and it has shone a light on this gaping black hole in medical research.
If we have the biomedical research then this changes everything; there can be an aetiology/cause; a pathophysiology/underlying disease mechanism; this means it can be taught it medical schools; Drs will have something to relate to and offer more care and actually believe it exists; this will then filter up to the public and stigma, prejudice and dismissal will reduce, the culture will change; then there’s actually hope for a treatment and possibly cure.
Part Two - Coming Soon
[1] Stenhoff AL , Sadreddini S , Peters S , et al Understanding medical students’ views on chronic fatigue syndrome: a qualitative study. J Health Psychol 2015;20:198–209. doi:10.1177/1359105313501534
[2] Thomas MA , Smith AP Primary healthcare provision and chronic fatigue syndrome: a survey of patients’ and general practitioners’ beliefs. BMC Fam Pract 2005;6:49. doi:10.1186/1471-2296-6-49
[3] Bowen J, Pheby D, Charlett A et allChronic fatigue syndrome: a survey of GP's attitudes and knowledge. Fam Pract 2005;22:389–93. doi:10.1093/fampra/cmi019
[4] https://www.bbc.com/future/article/20210609-how-long-will-long-covid-last
[5] Chitnis A, Dowrick C, Byng R. Guidance for health professionals on medically unexplained symptoms (MUS). Royal College of Psychiatrists. January 2011. http://www.rcpsych.ac.uk/pdf/CHECKED%20MUS%20Guidance_A4_4pp_6.pdf (accessed on 27 Apr 2016)
[6] gp_GUIDE_V_2_LEAFLET_22_MAY_14
[7] https://www.parkinsons.org.uk/sites/default/files/2017-12/northernirelandnursereport.pdf
[8] https://www.macmillan.org.uk/cancer-information-and-support/get-help/physical-help/cancer-information-nurse-specialist?gclid=cj0kcqjw3f6hbhdharisad_i3d9h87rljm_sb8ojg0kxc6wsc3abu8xkjer4lmxfifpk5v78mmrvj2kaarhlealw_wcb&gclsrc=aw.ds
[10] https://www.disabilityrightsuk.org/understanding-equality-act-information-disabled-students
[11] https://www.usnews.com/news/health-news/articles/2021-07-26/long-covid-can-be-a-disability-biden-administration-says
[12] https://www.usnews.com/news/health-news/articles/2021-04-15/covid-long-haulers-could-change-the-disability-system
[13] https://fraudlisting.com/index.php/about/
[14] https://petition.parliament.uk/petitions/582266
[15] Roberts E, Wessley S, Chalder T. Mortality of people with chronic fatigue syndrome: a retrospective cohort study in England and Wales from the South London and Maudsley NHS Foundation Trust Biomedical Research Centre (SLaM BRC) Clinical Record Interactive Search (CRIS) Register. Lancet 2016;387:1638–43. doi:10.1016/s1040-6736(15)01223-4
[16] https://www.wbur.org/hereandnow/2021/06/28/coronavirus-long-hauler-crisis
[17] https://www.meaction.net/2019/01/08/how-does-me-research-fare-check-out-these-piecharts/
[18] Dancy CP, Friend J. Symptoms, impairment and illness intrusiveness—their relationship with depression in women with CFS/ME. Psychol Health 2008;23:983–99. doi:10.1080/08870440701619957
[19] https://me-pedia.org/wiki/Biopsychosocial_model
[20] https://me-pedia.org/wiki/Michael_Sharpe
[21] https://www.cell.com/action/showPdf?pii=S1471-4914%2821%2900134-9
[22] https://www.nice.org.uk/guidance/indevelopment/gid-ng10091
[23] https://www.bmj.com/content/373/bmj.n1559/rr-12
[24]https://valerieeliotsmith.com/
[25] https://blogs.bmj.com/bmj/2021/06/23/how-power-imbalances-in-the-narratives-research-and-publications-around-long-covid-can-harm-patients/