



Tin Foil Hat Territory? The Gupta Program, the Lightning Process and the BPS in Long Covid and ME.
How brain retraining therapies intersect with the biopsychosocial model

This response to the wide-ranging concerns about brain retraining such as the Gupta Program and Lightning Process aims to inform patients and medical practitioners about the controversies surrounding these programs. We also draw links to the often unrealised connections between the brain retraining model and the biopsychosocial model, often used in clinical practice for ME and Long Covid.

Concerns from the Covid and Long Covid Community
In March 2020, when the Coronavirus Pandemic began, Ashok Gupta released a package called the 10-Day Coronavirus Challenge where:
Some of the tools in this program have been scientifically shown to reduce the chances of contracting an infection from a virus by over 80%.
The tools in his program are meditation, NLP, neural retraining and amygdala calming. A complaint was made to the ASA, and they responded by saying that there was a previous ruling against the owner or originator of the video and the video seems to fall within the scope of that ruling. Therefore the case has been passed to the Compliance Team.
Concern that Gupta, and Phil Parker founder of the Lightning Process, have jumped on the Long Covid bandwagon is well justified. They are attempting to treat Long Covid with no evidence, no industry standards and no protection for patients. While the disease mechanism has not been fully understood, it is highly unlikely it will be cured by pseudopsycho intervention.
The Gupta Program, as does the Lightning Process, aggressively lobbies those in the public eye, including those in the Long Covid field, such as Dr Tamsin Lewis, Dr Tina Peers, Gez Medinger, who then give publicity to their unproved theory, generating business and income. We saw recently that ex-Olympic rower Oonagh Cousins was approached to do The Lightning Process for free, although she brilliantly turned this on its head by exposing the treatment in a BBC Radio File on 4 by Rachel Schraer.
Historically we have seen Esther Ranzen and Martine McCutcheon endorse The Lightning Process. More recently Francesca Steele, a Times journalist, and the indefatigable Prof Paul Garner are avid propagators.
These affiliations give these brain retraining courses authority by association. They can pass as having expertise in treating Long Covid without even stepping into a lab or having any medical experience. This aggresive marketing tactic leads to exposure to a large audience.
Many patients are vulnerable and have little awareness of the previous controversies associated with brain retraining and are desperate to try anything to get better. Yet without research and training, offering a cure and charging sizeable sums of money to a community highlights brain retraining is patient exploitation.
Sponsorship of the Treat Long Covid Conference in 2021 by the Gupta Program raised concerns in the Long Covid Community that a pseudoscience organisation with a controversial and unproven treatment was being pushed to Long Covid patients.

Isabel Carrasco Sáenz notes:
Pseudoscience getting mixed up with real science. Very worrying. Gupta is sponsoring this conference. Don’t researchers have respect for their own work? How can hours and hours of lab work be at the same level as these ‘therapies’?
Peers even states on the front page of the Gupta website:
I now recommend the Gupta Program to all my patients as I believe that it plays a key role in their recovery.
Recommending ALL your patients to another expensive program which is unproven for Long Covid is dubious. Long Covid and MCAS, the two main conditions Peers treats, are complex and have many different symptoms; how would one justify each patient needing the Gupta Program?
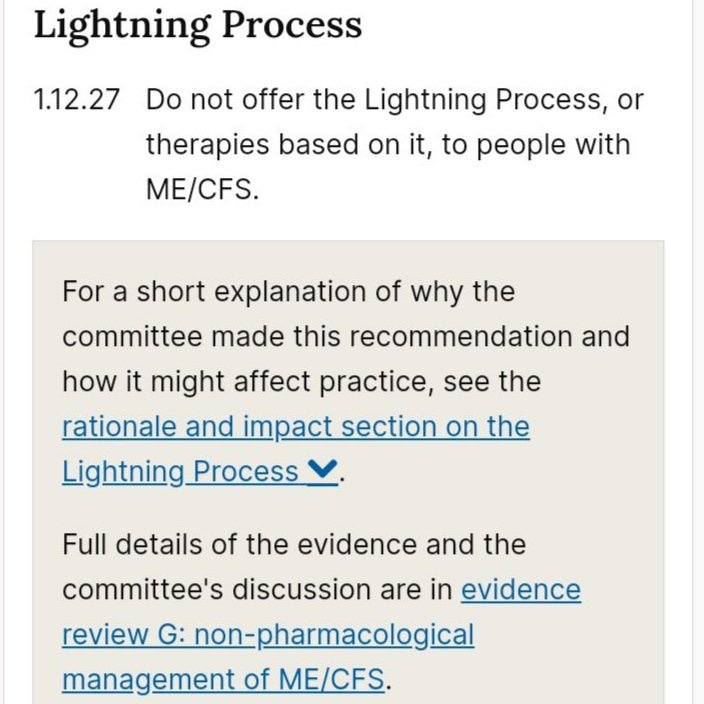
There are NICE guidelines for Long Covid, yet they do not protect patients from the Lightning Process or the Gupta Program. It would be sensible to infer the guidelines for ME/CFS (and revise the Long Covid guidelines) due to the overlapping symptoms and the mutual risk of relapse from PEM. Up to 89% of those with Long Covid have been surveyed as having PEM. As these programs often disregard pacing they are not safe for many patients. The draft NICE guidelines for ME/CFS states:
Do not offer people with ME/CFS therapies derived from osteopathy, life coaching or neurolinguistic programming (NLP) for example the Lightning Process. 1.11.16.
The commissioned NICE Guidelines also clearly state:
Historical and Present-Day Controversy within the ME Community

The Gupta Program and Lightning Process use the deeply controversial brain retraining methods that have caused immense problems in the ME community. This field can also be categorised under discredited psychological and behavioural therapies and mind-body treatments. None of which have strong empirical evidence. If you are not in this field, it is easy to not be directly aware of the hurt, false hope, money lost and patient harm inflicted on patients with ME.
I crashed really hard from doing Gupta and put it aside because I didn't understand the theory. I rarely have negative thoughts about anything, let alone being sick. I do have physical signals that modulate my behaviors and I'm not sure I want to turn them off. Jen Brea
Other brain retraining outfits include DNRS Dynamic Neural Retraining System, Alex Howard’s REACT, and ANS Rewire.
There is significant overlap in the theories of brain retraining and the biopyschosocial model used for ME established by the Wessely School. Both assume there is no organic disease process, the brain is deregulated and creating systems as a warning and can be treated with behavioural psychological techniques. In other words it’s a software not a hardware problem. Very much like the FND (modern day hysteria) hypothesis.
This (false) paradigm of the Wessely School, PACE trial and the brain retraining methods have prevented serious biochemical medical research into post-acute viral illness. We need immunologists, not psychiatrists and charlatans!
The underlying disease mechanism is not understood in ME because for decades psychiatrists and psychologists have fought for ME to be only in their field, which has dominated funding, research, clinical guidelines and medical insurance.
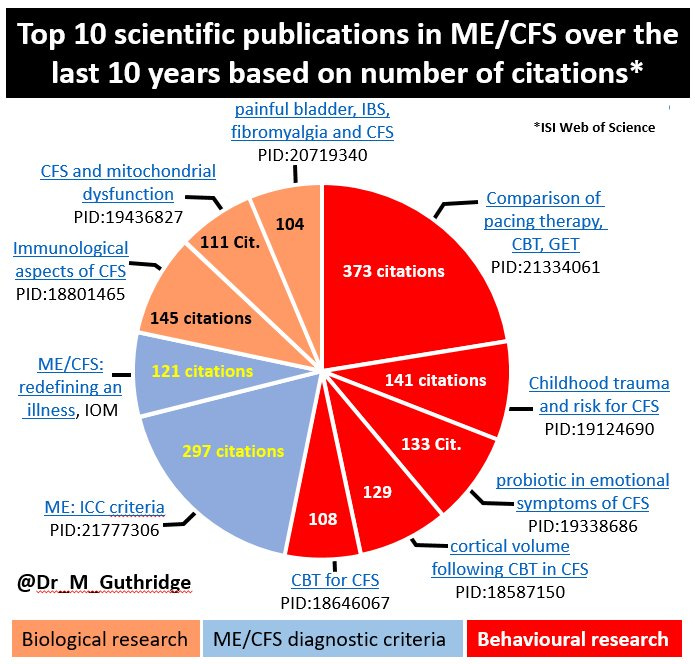
Dr Mark Guthridge collated figures that showed in 2018 ME had the worst quality of life and the least scientific studies and the least clinical trials. He shows in pie charts how the biopsychosocial school had dominated funding for research into ME for the previous 10 years. The top 5 influential papers were also in behaviourist research. He also reiterates that the BPS model has major flaws in its methodology that have been covered by The Lancet, The US Institute of Medicine the INAMI report in 2006 and recent meta-analysis (Malouff et al., 2008) of the efficacy of CBT in treating CFS found an effect size of d = 0.48 (95% CI 0.27–0.69).
The BPS (biopsychosocial) approach to ME established its dominance through the PACE trial, which is a largely unknown medical scandal, equivalent to Andrew Wakefield, MMR and autism, the Infected Blood and Post Office Scandals.
The history of ME remains one of the worst examples of unacknowledged institutional abuse in modern times. Valerie Eliot Smith
Patients campaigned for 5 years for the full data to be released and it was found to be substandard, with the researchers making up data to fulfil their hypothesis.
the height of clinical trial amateurism, Dr Bruce Levin, Biostatistician of Columbia
I’m shocked that the Lancet published it…The PACE study has so many flaws and there are so many questions you’d want to ask about it that I don’t understand how it got through any kind of peer review. Prof. Ronald Davis of Stanford
an unblinded trial with subjective outcome measures. That makes it a non-starter in the eyes of any physician or clinical pharmacologist familiar with problems of systematic bias in trial execution. Prof. Jonathon Edwards of UCL
Long Covid would be better understood if these delays had not happened. Advocating psychological methods is part of the problem, not the solution.
Psychological medicine has dominated post-acute viral conditions for four decades. The history of the treatment of ME also shows how ‘cures’ such as the Gupta Program and Lightning Process have been allowed to come into existence. They are an extension of this flawed paradigm as they use psychological methods to treat ME and other conditions including Long Covid.
The Biopsychosocial Infiltration into Long Covid
There has been a worrying trend of psychiatrists and other therapists involved in treating ME who are members of the Wessely school coming over into the field of Long Covid due to similar symptoms. The battle that has occurred within the ME is now being transposed into Long Covid.
Established figures in this biopsychosocial school such as Michael Sharpe, Paul Garner, Trudy Chalder, Simon Wessely and Peter White are all active in the media and trying to reestablish their disproven paradigm for psychological treatments such as CBT and GET for Long Covid.
An article by George Monbiot is an important read. Sharpe accused Monbiot of spreading Long Covid simply by talking about it. Simon Wessely, leader of the Wessley School chaired a committee on Long Covid (more details in this article); Michael Sharpe is back at Oxford and set up the Long Covid Clinic, and press articles are being published by leading figures of the school.
Dr Charles Shepherd, Hon Medical Advisor of the ME Association states:
NICE has warned that their current recommendations regarding GET for ME/CFS should not be transferred to people with Long Covid. We hope that this new cohort of post viral patients with Long Covid will not have to suffer the same mistakes that have been inflicted on people with ME/CFS
Despite this appearance of open debate, a clear scientific consensus has been reached. The NICE draft guidelines (November 2020) state:
If anyone deserves an apology it is the people with ME/CFS, many of whom have experienced years of being told that their symptoms are “all in the mind” and given no meaningful medical management – mainly as a result /of the dominance of the psychosocial model of causation. As a result, progress involving biomedical research into the underlying cause of ME/CFS has been severely hampered.
David Tuller in his virology blog states
For months, Professor Sharpe and his colleagues have been deploying the Long Covid phenomenon in a campaign to shore up their cherished but collapsing CBT/GET approach to ME/CFS and related conditions.
The point here is that it is not just Sharpe and his colleagues it is also the Gupta Method and Lightning Process that are found on the same principles: psychological treatments for a biophysical condition. They are trying to establish themselves in the Long Covid world without justification.
Advertising Violation
The ME Association does not recommend that people with ME take the Gupta Program. In September 2018 the ME Association reported their concerns to the ASA – Advertising Standards Agency. Dr Charles Shepard wrote:
In relation to the Gupta Programme, this is not a form of treatment that we recommend, and we welcome the fact that the ASA has taken this action in relation to the way it is being advertised to the general public.
The complaints were:
The complainant challenged whether the claims that the Gupta Programme could treat the following conditions were misleading and could be substantiated:
“Fibromyalgia”;
“Chronic Fatigue Syndrome (CFS) or ME”; and
“Electrical Sensitivities
All three complaints were upheld with the evidence produced by the Gupta Program seen as insufficient. Action:
We told Harley Street Solutions Ltd not to state or imply that the Gupta Programme could treat “Fibromyalgia”, “Chronic Fatigue Syndrome (CFS) or ME” or “Electrical Sensitivities”. We told them to ensure that they held substantiation for any similar claims relating to medical conditions or symptoms. ASA
Therefore, there should be no advertising or reference on the Gupta Program website that this method can treat these conditions. Seeing that about half of people with Long Covid meet ME criteria it is logical it can’t treat Long Covid as well. (well no illness to be fair!)
Mistakes Repeated
It is vital to not repeat the mistakes that were made with ME in Long Covid. It was through the faulty belief established through Behavioural Cognitive Psychology (Wessely School) that ME was caused by deconditioning and patients had false illness beliefs based on fear that prevented them from being active. Therefore, keeping themselves in a vicious circle of avoidance. ME was perceived to be a disease of psychiatric origin, mass hysteria.
This is also known as the biopsychosocial model (BPS). Therefore, GET (Graded Exercise Therapy) was prescribed to re-condition them and CBT to help them change their negative thought and emotional processes about exercise. While on this programme, physical and diagnostic tests are also to be actively avoided. Receiving benefits or sick pay was also discouraged, as this is seen as an obstacle to recovery.
We nee to be vigilant and educated to spot this charlatanary. We need therapeutic treatments that actually work and stop gaslighting those with post-acute viral disease.
Intersection in Paediatrics
One of the clearest intersections between Long Covid, the Lightning Process and ME is Prof Esther Crawley. She led the SMILE trial, investigating the Lightning Process for children in ME, published in 2017. The trial was heavily criticised as unethical and problematic. This included outcome swapping, the initial outcome was school attendance but was swapped to a subjective questionnaire, the SF-36. Phil Parker the Lightning Process ‘guru’ was involved and data was withheld from the public.
Yet we still have Crawley involved in the paediatric Long Covid study CLoCK. A study that is yet again investigating psychosocial factors in children for the perpetuation of their symptoms.
The worst-case scenario of inferring that abnormal psychology is a contributing factor in Long Covid and ME is that parents and children get blamed for their illness. Opening the door for social service referrals and institutional abuse. It is concerning that leading figures in the Long Covid and ME charity world have engaged Esther Crawley as a paediatrician for their families.
Treats MUS (Medically Unexplained Symptoms) and conditions with no measurable biomarkers
It is concerning and suspicious that Gupta and the Lightning Process (and the BPS model) pretty much only treat MUS (Medical Unexplained Symptoms) and conditions not treated or well understood in mainstream medicine and with no measurable biomarkers.
These include ME/CFS, Fibromyalgia, Mold, IBS, MCAS, Chronic Pain Syndrome, Long Covid, Anxiety, Adrenal Fatigue, SIBO, CIRS, Burnout, POTS and Multiple Chemical Sensitivities. Many therapists primarily see these MUS as psychosomatic conditions or manifestations of mental illness due to the way they are presented in medicine. Yet, it can also be seen as the height of medical arrogance to assume it is a mental illness because the aetiology has not been found.
Where is the evidence that these conditions are all connected and are different manifestations of the same Amygdala and Insula hypothesis? These conditions are often misunderstood and seen as having a psychological origin and not a genuine disease pathway. Maybe we should be looking in people’s bodies, at pathophysiology, not flitting about in non-falsifiable la la land?
Why do these approaches not primarily treat Cancer, Lupus, MS, Parkinsons? It would be absurd and insulting for patients with these conditions to be only treated and offered cures with brain retraining, CBT, NLP, rehab or Neuroplasticity. Why should sufferers of the illnesses Gupta and Parker claim to cure have to go through this either?
Just because an underlying disease mechanism has not been found does not mean it does not exist.
The false hypothesis of ‘symptoms without disease’

The Gupta Program puts forward a ‘symptoms without disease’ hypothesis: symptoms are caused by an overactive/reactivity in the brain that is unrelated to the original illness which is now gone from the body.
This ‘symptoms without disease’ is an extension of the work of the Wessely School. This school hypothesised that ME was psychiatric and had no disease mechanism in the body. It therefore needed to be treated with CBT, i.e. psychological methods to overcome faulty emotional and mental thinking/processes.
Michael Sharpe claims:
it is not a particular biological process, but rather specific psychological and behavioural mechanisms that are the common factors determining the clinical characteristics of the syndrome.
The Gupta Program employs a similar treatment program to CBT (changing thought processes and calming down the emotional system) although based more on NLP and is framed as neuroplasticity. This is the wrong paradigm to address serious illness and should be challenged. The website clearly states that after the original illness has gone the patient is left with symptoms but no underlying disease mechanism.
Magical Thinking and Patient Blaming

Brain retraining and psychosomatics often claim that if you aren’t cured you didn’t try hard enough. There is serious patient danger with these models. It roots the aetiology of the illness in the false beliefs and emotional trauma or stress of the patient.
The Gupta Program and Lightning Process involve visualizing yourself well and interrupting thoughts about your illness with hand signals and phrases such as “soften and flow” and “stop, stop, stop”. This is clearly an attempt to treat a physical illness with psychological methods. It is therefore the efficacy of the patient in carrying out these procedures that determines the cure. So the cause and the cure are down to the agency of the patient.
No one blames an individual for getting cancer or MS or gives them psychological techniques primarily to treat and cure them or blames them for not recovering if they do not rewire their amygdala.
In Anthropology, this is termed “magical thinking” and discussed at length by Levi-Strauss. In medicine, it is often called ‘mindset medicine’. This is where changing our thinking will change our reality and, therefore, our illness. This should not be a method in modern medicine and is absurd. If this were the case, then all illnesses or difficult situations would easily disappear. Yet, this is the stance that the Wessely School took through the treatment of CBT, as did the NLP and Brain Retraining of the Gupta Program and Lightning Process.
Institutional Medical Misogyny – Reinventing the Hysteria Paradigm

ME, Lyme disease and Long Covid as well as other autoimmune conditions that brain retraining claims to treat predominantly affect women. The historical pattern of this paradigm is hysteria. Women’s pain is often more likely to be classified as emotional or psychological in origin and requires emotional or psychological treatment. This is investigated in depth in Gabrielle Jacksons ‘Pain and Prejudice: A call to arms for Women and their Bodies’ and in Elinor Cleghorns’ book ‘Unwell Women: Myth and Misdiagnosis in a Man-made world’.
Early onset Parkinson’s in women is still more likely to be classed as ‘emotional’. MS before the physical disease origin was discovered was also seen as an onset of hysteria.
The medical world does not tend to use the word hysteria now, the terminology has changed to ‘emotional’, ‘psychological’ ‘based in the neurological system, ‘overactive amygdala’, ‘sympathetic nervous system arousal’, ‘anxiety’ or ‘stress’. In medical diagnosis hysteria became conversion disorder and then FND.
Any treatment program that uses calming methods is propitiating the hysteria program by essentially saying that if we calm down, we will be cured. That illness caused by faulty emotional and mental processing based in the nervous system (previously called hysteria) through calming will go away.
Essentially the Gupta Program and Lightning Process is a heavily disguised hysteria paradigm that is repackaged in the language of neuroscience. The Industrial Hysteria Complex is still with us.
Cult-like Behaviour

Both the brain retraining gurus and the BPS model fit into cult behaviour as James Randi states:
The first thing a cult does is tell you everyone else is lying
Both are guilty of this. Casting the unbelievers as ‘activists’ or even Phil Parker’s ‘anti-recovery activists’. Both at their core ask you to disbelieve that there is an organic disease process and they expect recovery from psychological intervention. It’s literally like aspiring to magical powers through thought that can heal you.
Secrecy is a major factor too. There are threats and strict measures for not sharing the methods used and staying off social media. Mixing with those who are still ill is also off the cards. It’s fire and brimstone territory folks. Yet, the reality is they are brainwashing you to ignore your symptoms. This is dangerous as activity and pushing out of the energy envelope for those with PEM can lead to deterioration.
The Wessely school and brain retraining gurus are based around a leader who cannot be wrong or questioned without castigation; they are sure they possess the truth and are vitriolic if challenged. The Gupta Program and Lightning Process have their floor stop maps that you endlessly parade around trying to rewire yourself and the Wesselyites have their CBT processes to stop you from continuing your harmful ‘false illness beliefs’ and abnormal psychology. There is no room for doubt.

Floor Map ‘inspired’ by Brain Retraining
Psychological Primary Treatment and not Secondary and Supportive
In an ideal world, counselling, mindfulness and stress management should be given to those with chronic illness – this can be very helpful. Stress undoubtedly can cause physical symptoms in the body. Yet this is very different to saying that stress, trauma or faulty emotional and mental patterns are the aetiology of a disease and the underlying disease mechanism and therefore the patient needs mindfulness-based techniques and a change in thought processes to be cured.
You can not imagine that a cancer patient or Muscular Dystrophy patient to be only offered psychological cures This is what has happened to ME patients for decades. This is also the basis of the therapies offered in the Gupta Program such as visualising yourself better, repeating phrases such as “soften and flow” and interrupting thoughts about your illness with gestures and phrases such as “stop stop stop” and other CBT methods of thought stopping.
Classic Pseudoscience
The Gupta Program and The Lightning Process are pseudoscience, as they assert to be scientific; its allegedly established facts are presented as justified true beliefs and it asserts that its established facts have been justified by genuine, rigorous, scientific methods.
Other concerns are that it uses obscurantist language, and technical jargon to give claims the superficial authority of science.
All of the brain retraining methods piggyback on the newly emerging field of Neuroplasticity and draw on the authority of Neuroscience terminology. All of this is unproven, as Dr Camilla Nord, neuroscientist clearly states as “neurobollocks”.
I’m afraid now we’ve strayed very, very far from neuroscience,” Dr Nord says, calling this an “abuse” of scientific terms.

Long Covid Clinics
Even now the Long Covid Clinics are primarily based on rehabilitation both physical and psychological just as the old Wessely School instituted CBT and GET. Yet it is a murky mix as to why psychological rehab is given.
We are often given different reasons for having psychological rehab from the old school BPS, that it’s for a fear-based false illness belief. Sometimes it’s stated that it’s soley for supportive measures. Yet, often this psychological intervention is connected to symptom reduction.
It’s become a confused half-way house of double-speak with a hall of mirrors thrown in. We can see clinical practice is still influenced by the Wessely model. We know BACME, a problematic organisation, founded by Esther Crawley, is connected to Long Covid clinicians. The 2 clinical co-chairs of the Long Covid Allied Health Therapies Clinical Network, Chinea Eziefula and Rebecca Livingstone presented at BACME 2024.

Tied into that we have the predominant and problematic biopsychosocial model of pain involved. It’s a mess and at times one can hardly see the difference between Long Covid Clinics and a brain re-training course.
The recent slides from the 2024 NHS Conference were a wild west hodge podge of behavioural slurry. It seems that each clinic can essentially do what it likes.
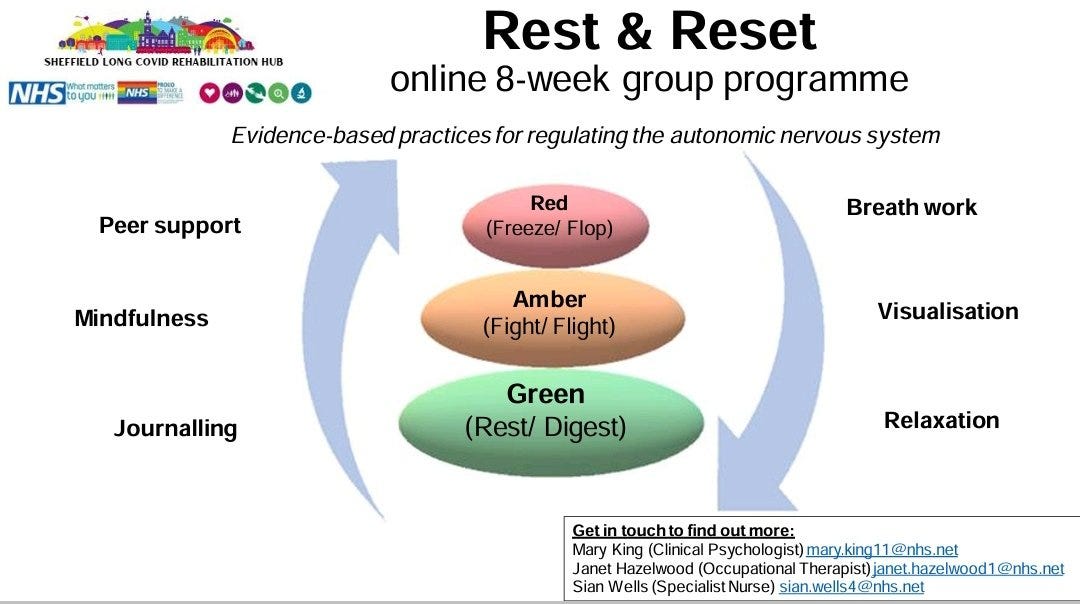
Here is the Sheffield Reset program offering the same hypothesis as brain retraining, an overstimuated nervous system, (which is also pseudoscientific polyvagal theory) which can be calmed through treatment options based on mindfulness and psychological intervention. This isn’t holistic psychological therapy designed to support and deal with the trauma of devastating life changes due to chronic illness, this is symptom based.
Another example is Sussex Long Covid Clinic stating in 2024 that Covid does not cause structural damage to the brain (counter to evidence) and that psychoeducation is therefore justifiable as a treatment. Here we have the ‘symptoms without disease’ approach. It is quite a leap to state that if we reduce anxiety about our symptoms that Long Covid difficulties can be reversible.

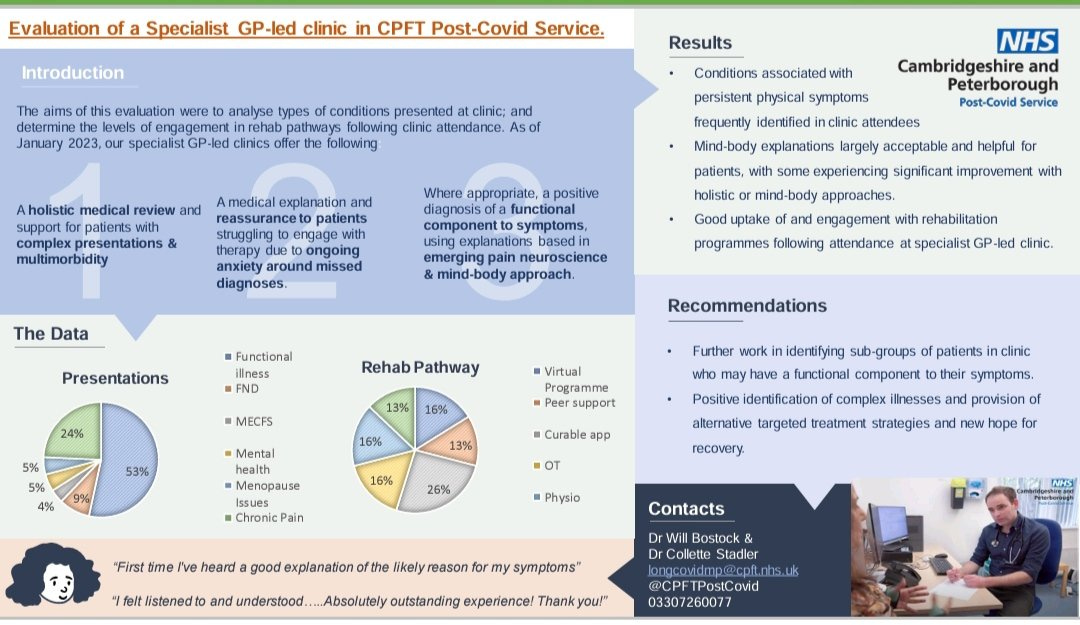
There is an ingrained culture in the NHS and in Long Covid Clinics that illnesses that are not understood by the system are functional. This isn’t a polite term. It means that there are ‘symptoms without disease’. Sound familiar? In other words psychosomatic. Here Cambridgeshire Long Covid Clinic stated that 53% of patients has a functional illness with 9% having FND, the modern name for hysteria.
Here we can also see how validation and being believed about your symptoms isn’t all that it’s cracked up to be at the bottom right of the image. Yet, even with what the research is telling us, we need more than ‘validation’ that our illness is real. Especially when ‘real’ can be so misconstrued. (Symptoms real but no real brain pathology love)
But, it is important to remember, that whatever the reason given, we are still left with the same treatment, behavioural and psychological, that doesn’t work to address the underlying disease pathology. It just feels like a distraction-based sleight of hand to keep the same old paradigm in place. It is likely that even the health professionals responsible are so tangled up in words with double meaning, influence and intention that no one knows where they stand. We don’t have effective treatments because of this model so why risk perpetuating it because there isn’t anything else? The deliniations for patient safety are not clear enough for harm not to be done.
Conclusion
Trying to treat illnesses such as ME, Chronic Pain, or Fibromyalgia, especially women, with emotional and psychological techniques is troubling and wrong. Whether it is via commercial brain retraining ‘gurus’ or NHS clinical care. Funding and focus on actual pathophysiological research is urgently needed to prevent long-standing issues recycling once again. Yet this habit is deeply ingrained in society and medicine.

There is a case for psychiatrists and psychologists offering primary treatment to stay away from the medical fields such as ME, Long Covid, and Fibromyalgia. Just because a condition is not understood doesn’t mean it needs to be treated with emotional methods. What is needed is better research from immunologists, virologists and other medical fields that might be able to shed light on the understanding mechanism. Until this is discovered, all you are giving is a sticking plaster.
This doesn’t mean we shy away from acknowledging or giving psychological support for the medical trauma and neglect that millions have suffered. But this isn’t the type of psychological support that is usually on the table in the NHS or through brain retraining. Both are inherently linked with the treatment of symptom causation or sustaining symptoms.
Like other conditions with ineffective treatment methods (Long Covid, ME/CFS, Lyme) there is growing pressure from society and the medical community for them to be more thoroughly researched, more effective care given and for physical biomarkers and treatments to be found. We need to move away from giving psychological primary care and funding and researching these chronic conditions that create years of pain and suffering to mainly women who have been ignored.
It would be safer for patients to be referred to independent councillors who can give long-term trauma-based support. Yet this is far from the cheap, mass-producible 6-week course often rolled out by the clinics. We need clinics to get on with diagnosing and treating the same intersecting conditions that often arise with Long Covid, such as ME, POTS, EDS and MCAS. (But there are no guidelines for all of these conditions, so we are back to square one).
Let’s be on the right side of history and do everything we can to move away from the psychogenic paradigm and research the pathophysiology.
A summary of sources of the harms of brain retraining/rewiring.
Coda
Further analysis of studies promoted by Gupta (if interested)!
Within pseudoscience, there is often ‘scientific evidence’ to validate the given theories but in reality, this is not rigorous and sufficient evidence it just sounds good. We find this with the Gupta Method and Lightning Process.
So let us examine the scientific proofs given by Gupta and their criticisms.
Let’s consider first what the ASA (Advertising Standards Agency) wrote in 2018 about the claims and evidence presented to them.
When asked for a response the Amygdala Retraining/ Harley St Solutions claimed they had conducted clinical trials on their protocol and it could substantiate it could be used to support CFS/ME and Fibromyalgia. They produced 2 published studies and a draft manuscript for the 3rd study.
The first study was on fibro and CFS and was peer-reviewed in a journal focused on complementary medicine. It was a single-blinded study and compared the efficacy of amygdala retraining alongside ‘standard care’ – which was a 1.5-day course in CBT and GET. Over half did not complete the study so out of the total 44 participants only 21 completed it, and only 7 from the amygdala retraining group did. This shows significant limitations with such a small case study. The ASA concluded that the study did not substantiate claims that amygdala retraining could treat Fibromyalgia or CFS.
The 2nd Study was for CFS only and was an internal clinical audit. It was published in a peer-reviewed journal focused on complementary medicine. As a clinical audit, it was not controlled, randomised or blinded. It was authored by the Director of Harley St Solutions (Ashok Gupta) who described the outcome of a 1 yr program. 27 completed the course. Again, we have a very small case study, researcher bias, and those who had invested financially in a program were also biased. The ASA stated that due to the limitation of an internal clinical audit the claims that the amygdala retraining process could not be substantiated.
The draft manuscript was from a Spanish randomised controlled trial which wasn’t published so it was not subject to peer review. The treatment delivery did not replicate the method of the Amygdala retraining course advertised. There were 64 participants, 22 in the relevant group and only 19 completed the study. Again this is a small sample size and it was not able to control for the possible influences of the individual therapist in each group. Again the ASA ruled that the trial did not substantiate claims made by Harley St Solutions.
Examining the study in September 2010 in the Journal of Holistic Healthcare again we see not a high enough case study, no randomisation, no control group, no controlling for other treatments or blinding to prevent researcher and sample bias.
We can conclude that the Gupta Program claims to be backed by scientific studies but under closer examination, they are not sufficient to be used as evidence. This is very concerning for the general public who may not have a science background and are being fooled into thinking what they are doing has genuine empirical evidence behind them. It is telling that the Program thinks that it can bring forward and back its claims with scientific evidence where anyone with any scientific training would know that these studies are not sufficient in the least. Combined with the claims that the Gupta Program could reduce your chance of catching the coronavirus by 80% we would conclude that Ashok Gupta is not a reliable source of information or evidence for his program.
In 2020 Gupta released on his website “New Study Shows Neuroplasticity ‘Brain Retraining’ program is an Effective Treatment for Fibromyalgia”. But again, let’s look a little closer at the details. On examination, we find that this is the same study that was presented to the ASA as evidence. There was a draft manuscript that hadn’t been published and is the Spanish study. Let’s look again at what the ASA said about the study: that it did not replicate the method of the Gupta Program; it was a small case study – 19 completed the study, and it did not control for the possible influences of the individual therapist in each group. The ASA have said that this paper does not give enough evidence to claim to treat or cure fibromyalgia.
Looking at the actual study, called ‘Mindfulness-Based Program Plus Amygdala and Insula Retraining (MAIR) for the Treatment of Women with Fibromyalgia: A Pilot Randomised Controlled Trial’ in the Journal of Clinical Medicine. The Journal is an open access Journal so not the most prestigious. I would begin by saying the sample size of 19 is far too small to make claims that the Gupta Program is an effective treatment for Fibromyalgia. The patients also continued to take their normal drug routine so we do not know if over this period they showed improvement from their other medical treatments. One of the major issues though is that we have 2 psychological treatments bundled together, mindfulness and Amygdala and Insula Retraining. This means we cannot know which is causing the effect.
Patients completed some practices included in the mindfulness-based stress reduction (MBSR) program that were added to the amygdala and insula retraining techniques (AIR)
Gupta’s method is based on Amygdala retraining this is the basis of his hypothesis and ‘cure’. If the study had just been done with Amygdala and Insula Retraining then it would have given us a clear indication. This is a logical fallacy: A+B→C, therefore A→C.
The researchers of the paper were contacted and did not know about the Gupta Program claiming that their paper gave credence to the Gupta Program. Dr Juan Luciano, lead researcher of the paper, replied:
I am really sorry to read this. We had no idea that Mr. Gupta was using our study for commercial purposes. On behalf of my colleagues, I can only assert that there is no personal relationship with Dr. Gupta nor commercial or financial interests with his program. That said, it’s really difficult to force him to retract. In my opinion, any legal intervention against Mr. Gupta is in the hands of the UK authorities. We are only academics/researchers attempting to provide the best empirical evidence of available treatments for fibromyalgia, CFS and other central sensitivity syndromes.
Ashok Gupta initially claimed it was ‘our study’
Our Ground-Breaking Study on the Gupta Program Published In The Prestigious Journal of Clinical Medicine. Giving Hope To Millions of Fibromyalgia Sufferers, as the First Randomized Controlled Trial Ever Published on a Neuroplasticity Program!
Yet that has now been removed from the webpage. It is clear from Dr Luciano that the study is not based on the Gupta Program or has any connection to the organisation.
Mindfulness might make you feel better about yourself and this is where the rub lies. Gupta has just jumped on the Mindfulness bandwagon and bought it into his treatment to try to make it sound more on-topic, acceptable and as a way to get published.
The study was for 8 weeks and Gupta claims on his website
so we expect even better results when used for a longer period
But there is no proof of this. This is a problem of replication as the study was not under the same conditions as the Gupta Program and other factors and conditions of the experiment might affect the results.
We contacted the ASA regarding the publishing of this study as “proof” of treatment and they responded:
We’ve assessed the ad you highlighted and from the information we have, we think the ad is likely to have broken the Advertising Codes that we administer and therefore will be taking steps to address the issue. We will explain your concerns to the advertiser and provide guidance to them on the areas that require attention, together with advice on how to ensure that their advertising complies with the Codes.
Great article, thanks for sharing it.
Had an abominable experience with the aforementioned Cambridgeshire LC clinic. Couldn't help but wonder if anyone was controlling their work. If someone had ever told me what I'd experience with them, I wouldn't believe them. Awful is an understatement.